Plus: Bernie Sanders' big spending plans
Court Rejects Trump Admin’s Medicaid Work Rules
A federal appeals court on Friday struck down the Trump administration’s approval of work requirements in the Arkansas Medicaid program, delivering a serious blow to the effort to impose more stringent rules for participation in the country’s primary health care program for the poor.
Upholding a lower court decision, a three-judge panel of the U.S. Court of Appeals for the D.C. Circuit ruled unanimously that the Department of Health and Human Services lacked the authority to approve work requirements, and that Trump administration officials had been “arbitrary and capricious” in allowing Arkansas to impose such requirements two years ago. The opinion was written by Senior U.S. Circuit Judge David B. Sentelle, a Reagan appointee.
Arkansas was the first state to receive permission to deploy Medicaid work requirements, which oblige aid recipients to work, volunteer or attend school for a certain number of hours each month in order to remain in the program. The Trump administration has now approved work requirements in 10 states, some of which have paused their efforts pending litigation. Nine other states are seeking approval.
Here’s what you need to know:
The court found that the Trump administration disregarded the purpose of Medicaid: The court affirmed that the primary purpose of Medicaid is to provide medical care to the needy, saying that it “is indisputably correct that the principal objective of Medicaid is providing health care coverage.” When it comes to making changes in the program, the court said that the secretary of Health and Human Services “is guided by the statutory directive that the demonstration must be ‘likely to assist in promoting the objectives’ of Medicaid.”
The Trump administration has attempted to justify the work requirements by referring to an alternative set of objectives, arguing that they would help people become healthier and financially independent. The court said those goals “are not consistent with Medicaid” and declared that the “text of the statute includes one primary purpose, which is providing health care coverage without any restriction geared to healthy outcomes, financial independence or transition to commercial coverage.”
The court said the work requirements have harmed recipients: “The record shows that the Arkansas Works amendments resulted in significant coverage loss,” Judge Sentelle wrote. “In Arkansas, more than 18,000 people (about 25% of those subject to the work requirement) lost coverage as a result of the project in just five months.”
The court criticized the Trump administration’s decision-making process: The judges were critical of Trump administration health care officials, including the HHS secretary, finding that they had failed to consider the potential loss in medical coverage that would result from the work requirements, despite warnings about such losses that emerged in comments during the public review process.
“Failure to consider whether the project will result in coverage loss is arbitrary and capricious,” Sentelle said. “In total, the Secretary’s analysis of the substantial and important problem is to note the concerns of others and dismiss those concerns in a handful of conclusory sentences. Nodding to concerns raised by commenters only to dismiss them in a conclusory manner is not the hallmark of reasoned decisionmaking,” the ruling says.
Critics claim a decisive victory: Critics of work requirements for recipients of public aid have long held that such efforts are thinly veiled attempts to prevent needy people from getting help they are legally entitled to receive. Sam Brooke, deputy legal director of the Southern Poverty Law Center, which challenged the work rules, said the “court confirmed that this administration’s effort to ‘explode’ Medicaid by converting it from a health care access program to a work program is arbitrary and illegal.”
What comes next: Nicholas Bagley, a law professor at the University of Michigan, said he expects all efforts to enforce state-level Medicaid work requirements to be suspended unless and until the Supreme Court reviews the case. “The Trump administration will probably appeal this decision to the Supreme Court, but it's hard to make a case for special urgency, especially since it's trying to slow-roll the constitutional challenge to the [Affordable Care Act],” Bagley wrote Friday. “So if the Supreme Court agrees to hear the case -- and I think it probably will -- we're talking about an argument sometime in the fall or winter, followed by a decision in late spring of 2021.”
Annual Health Spending for Privately Insured Hits All-Time High: Report
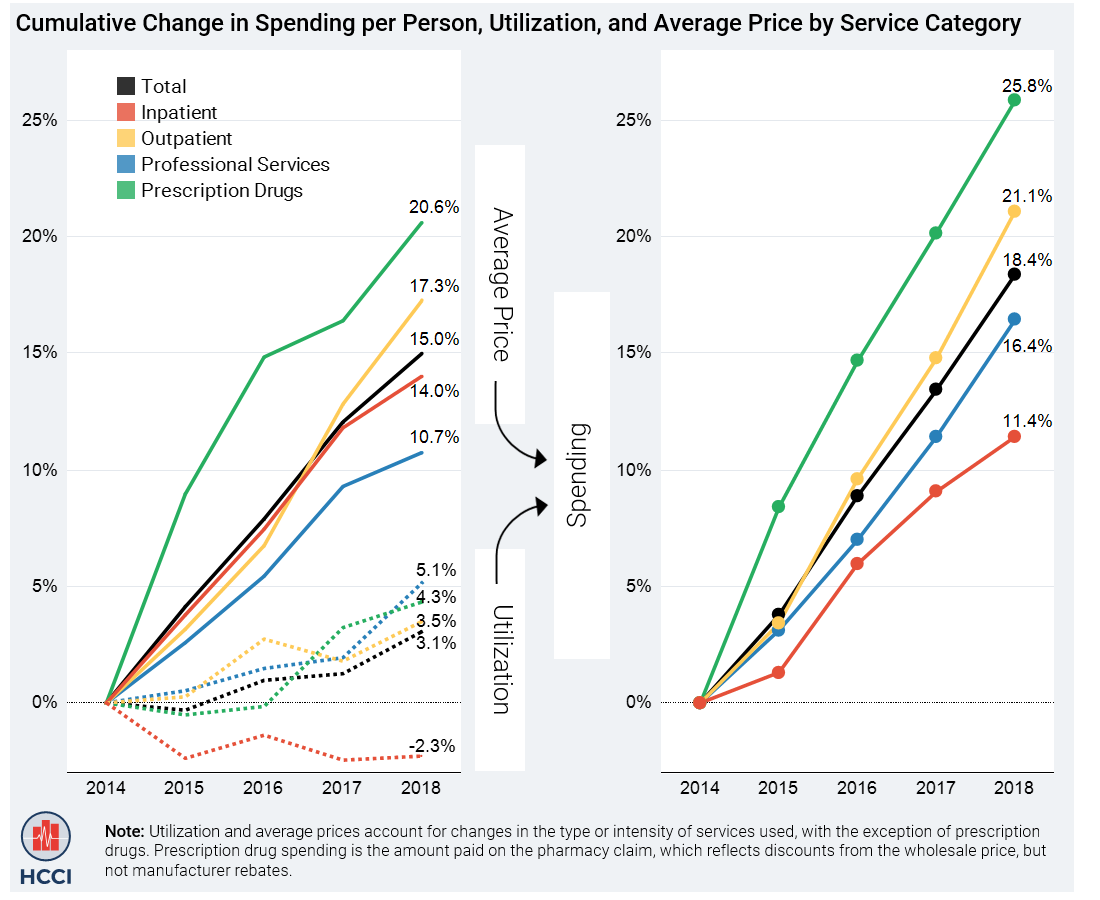
Average annual health care spending for people with employer-provided private insurance rose to an all-time high of $5,892 in 2018, according to the Health Care Cost Institute’s yearly Health Care Cost and Utilization Report, released on Thursday. Spending per person grew by 18.4% from 2014 to 2018, the report says, with about three-quarters of the increase due to rising prices rather than an increased use of health care services. In 2018, use of services edged up 1.8%, the first uptick in several years.
“Looked at another way,” STAT’s Ed Silverman writes, “from 2014 to 2018, per capita GDP in the U.S. grew annually at an average rate of 3.4%, while health care spending per person for those with employer coverage grew 4.3% on average. Meanwhile, per-person spending on prescription drugs grew at an average annual rate of 5.9%.”
Some other data points from the report:
- Health care spending grew 4.4% in 2018, the third straight year growth was above 4%.
- Out-of-pocket costs for people with job-based rose 14.5%, or $114, between 2014 and 2018. That includes copays, coinsurance and deductible payments, but not premiums.
- Prescription drug spending for those with private insurance rose by 26% over that period, outpacing cost increases in other categories (see chart below).
- Per person spending on drugs accounted for almost 20% of all health care spending.
- The average price of medicine climbed by almost 21%.
- Generic drugs accounted for 88% of all prescriptions, and out-of-pocket payments for generic prescriptions were less than one-fifth of such payments for brand-name drugs.
- Emergency room spending increased 32% over the five years studied.
- Spending on psychiatry rose by 43% over that span, driven mostly by increased use.
{kind=link}
Op-Ed of the Day: Health Care’s Three-Way Race for Your Money
The phenomenon of “surprise” medical bills — typically large, unexpected bills delivered to unsuspecting patients for services performed by out-of-network providers — is relatively new, and in Friday’s New York Times, physician and journalist Elisabeth Rosenthal takes a look at how they came to be:
“Surprise bills are just the latest weapons in a decades-long war between the players in the health care industry over who gets to keep the fortunes generated each year from patient illness — $3.6 trillion in 2018. ...
“Forty years ago, when many insurers were nonprofit entities, and being a doctor wasn’t seen as a particularly good entree into the 1 percent, billed rates were far lower than they are today, and insurers mostly just paid them. Premiums were low or paid by an employer. Patients paid little or nothing in co-payments or deductibles.
“That’s when a more entrepreneurial streak kicked in. Think about the opportunities: If someone is paying you whatever you ask, why not ask for more? ...
“So today your hospital and doctor and insurer — all claiming to coordinate care for your health — are often in a three-way competition for your money.”
Read Rosenthal’s full piece here.
Point-Counterpoint: Sanders’ Big Spending Plans
Sen. Bernie Sanders, the current frontrunner for the Democratic presidential nomination, has proposed ambitious plans — most notably, a transition to a Medicare-for-All system — that would dramatically increase the size of the federal government. The centrist Progressive Policy Institute estimated recently that Sanders has proposed more than $50 trillion in new spending, the most of any presidential candidate, and has laid out options for raising revenue to finance about half of that increase.
In a pair of newly published opinion pieces, USA Today’s editorial board debates such an expansion with Josh Bivens, director of research at the Economic Policy Institute, a progressive think tank. Here’s a summary of the arguments:
These proposals are a gift to Trump and the GOP: “Republicans know that large segments of the electorate would be repelled by Sanders’ vast expansion of government spending at a time when Uncle Sam is already running $1 trillion annual deficits and is more than $23 trillion in debt,” the USA Today editorial board says.
Sanders’ tax and spending plans aren’t politically feasible, anyway, so embracing them would only serve to lessen the chances of winning over suburban professionals, a critical bloc of voters. “For Democrats, this should pose a number of questions. Foremost among them: Why are they spending so much time debating these costly, unrealistic plans when they should be focused on preserving Obamacare protections and the rule of law?”
It’s time to tackle the problems the U.S. faces: Yes, Sanders’ plans are ambitious. “The key thing people should realize, however, is that these plans are largely not introducing new costs on American families,” Bivens writes. “Instead, they’re rearranging current costs already baked in, with an aim to managing them more fairly and efficiently.”
Medicare for All would replace our current premiums with taxes — and it could actually reduce the total costs of American health care, even as it gets more people covered, according to some analyses. And not tackling climate change now will only cost us and future generations more later. “The United States is an enormously rich country with hugely pressing problems stemming from a past generation of rising inequality and a future of climate change. Why would we not go for bold solutions?”
Read the USA Today editorial here and the Bivens op-ed here.
Your Prize for Making It Through the Week
Here’s a little Valentine’s Day gift from us to you: Health policy experts have been posting their holiday-themed poems to Twitter in recent days. Check out the hashtag #HealthPolicyValentines, our visit Kaiser Health News for a roundup of some of the best. Here’s one we liked:
Have a great weekend!
Send your tips and feedback to yrosenberg@thefiscaltimes.com. Follow us on Twitter: @yuvalrosenberg, @mdrainey and @TheFiscalTimes. And please tell your friends they can sign up here for their own copy of this newsletter.
-->
News
- Trump Weighing 10 Percent Middle-Class Tax Cut Plan – Politico
- White House Considering Tax Incentive for More Americans to Buy Stocks, Sources Say – CNBC
- Pelosi's Staff Huddles With Aides in Both Parties on 'Surprise' Medical Billing – The Hill
- Senate Democrats Pressure Trump to Drop Obamacare Lawsuit – The Hill
- Over 20 State Attorneys General Reject $18 Billion Opioid Settlement Proposal – NPR
- Space Force War Request Marks Budgetary First – Roll Call
- Trump’s Budget Steps on GOP’s New Climate Message – Roll Call
- U.S. Population Will Decline Faster Without Steady Immigration, Census Report Says – Washington Post
- Trump’s Story About Veteran’s Comeback Was Not Quite True – Associated Press
Views and Analysis
- Would ‘Medicare For All’ Cost More Than U.S. Budget? Biden Says So. Math Says No – Shefali Luthra, Kaiser Health News
- The Big Roadblock For Bernie Sanders' Agenda – Matt Fuller, HuffPost
- Labor Unions Aren't Sure About Medicare-for-All. That's Bad for Sanders and Good for Buttigieg. – Paige Winfield Cunningham, Washington Post
- To Fight Trump’s Medicaid Block Grants, Defense Isn’t Enough for Democrats – John Kitzhaber, Morning Consult
- Who’s Profiting From Your Outrageous Medical Bills? – Elisabeth Rosenthal, New York Times
- Here’s One Tax Every Candidate Ought to Back – Antonio Weiss, Bloomberg
- Why This Could Be the Last Year the Pentagon Pays for the Border Wall – Meghann Myers, Military Times
- Why We Can’t Cure Cancer With a Moonshot – William G. Kaelin Jr., Washington Post
- Democrats and Republicans Should Both Embrace This Common-Sense, Planet-Saving Reform – Washington Post Editorial Board
- Better Pay for Teachers Makes Perfect Sense. But Getting There Won’t Be Easy. – Jay Mathews, Washington Post
- The Rich Can Probably Escape New Laws on Inherited IRAs. But the Rest of Us Can’t. – Allan Sloan, Washington Post
- This Is How Scandinavia Got Great – David Brooks, New York Times
- ‘Parasite’ Paints a Nightmarish Picture of Korean Inequality. The Reality in America Is Even Worse. – Christopher Ingraham, Washington Post